Radiology guide
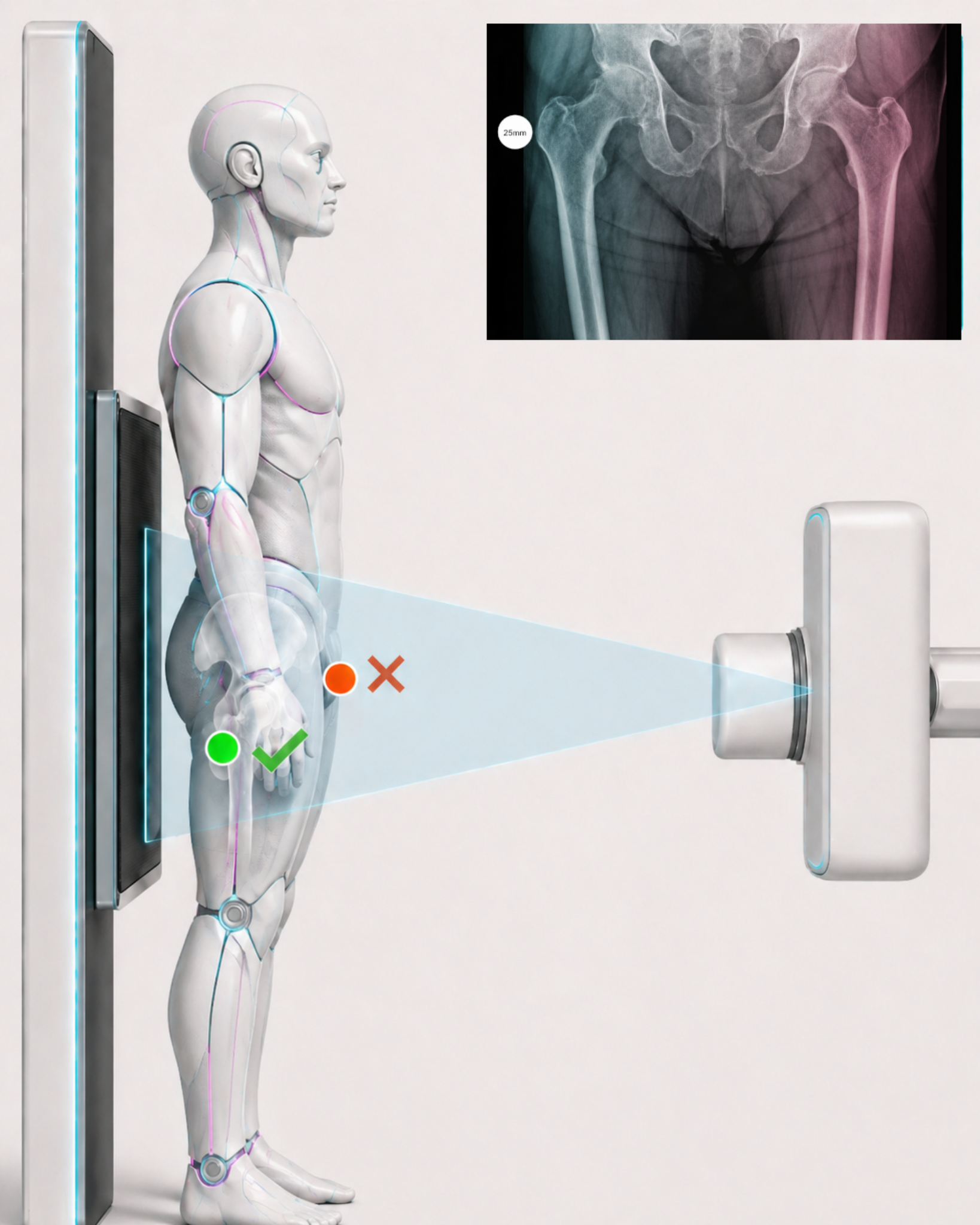
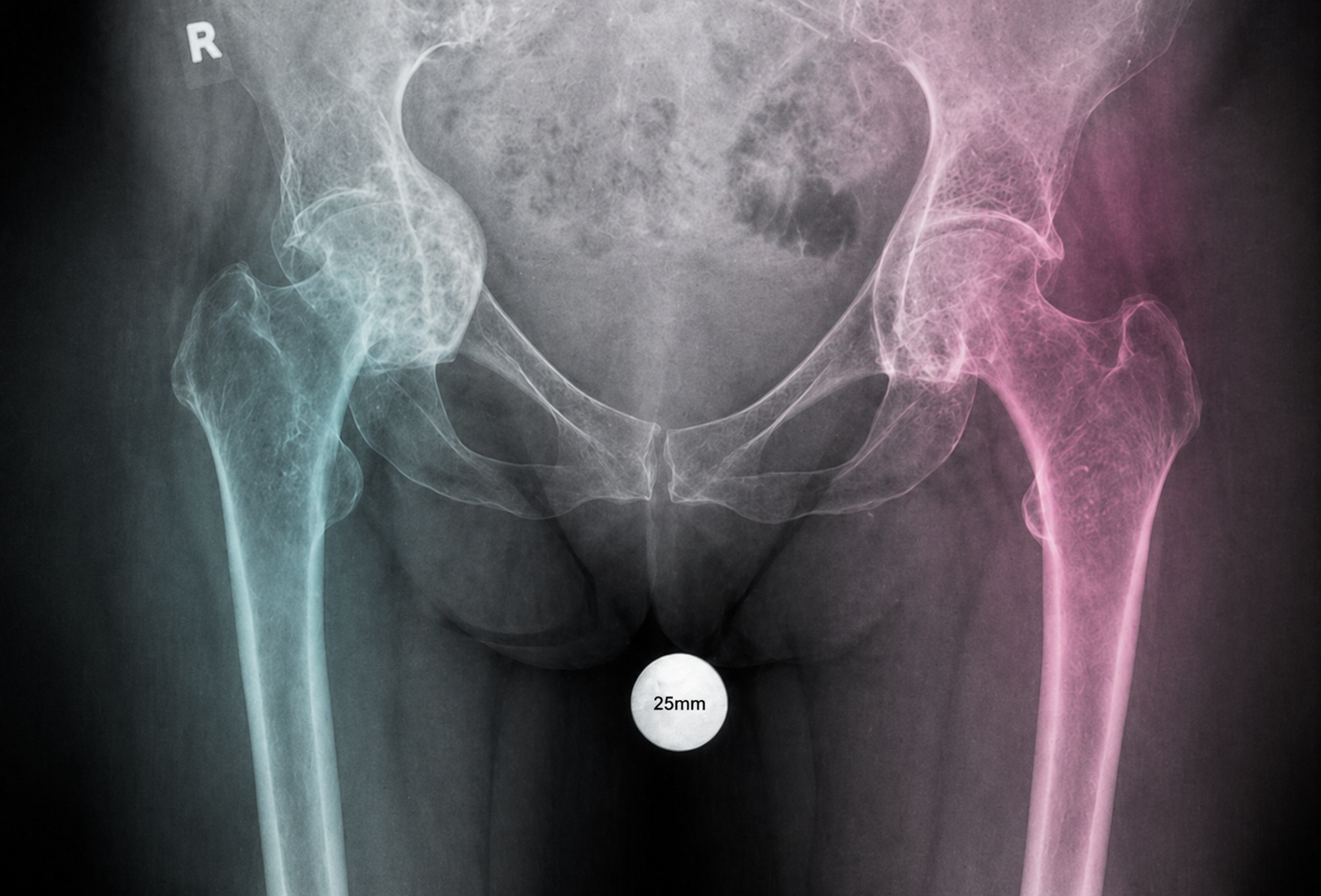
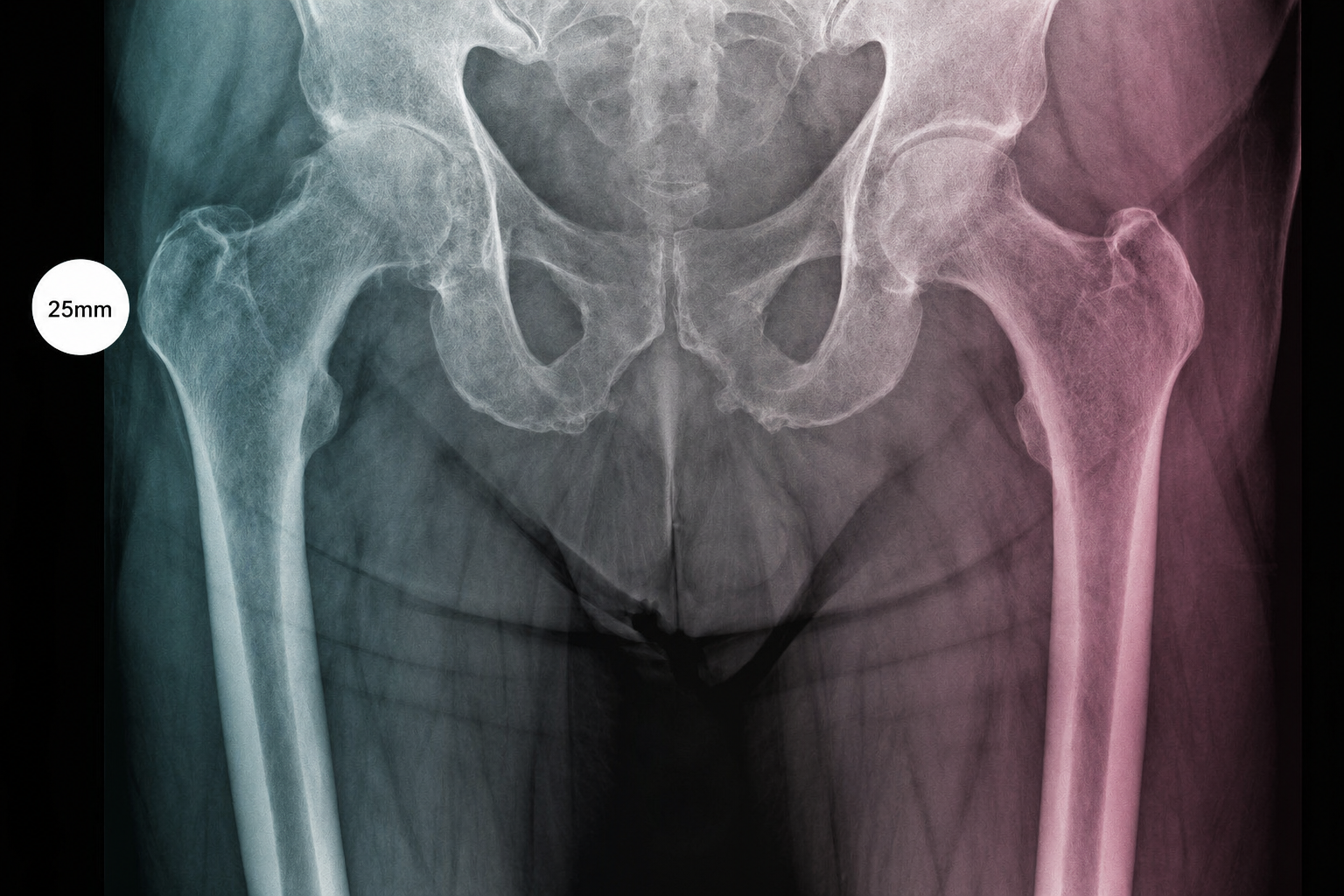
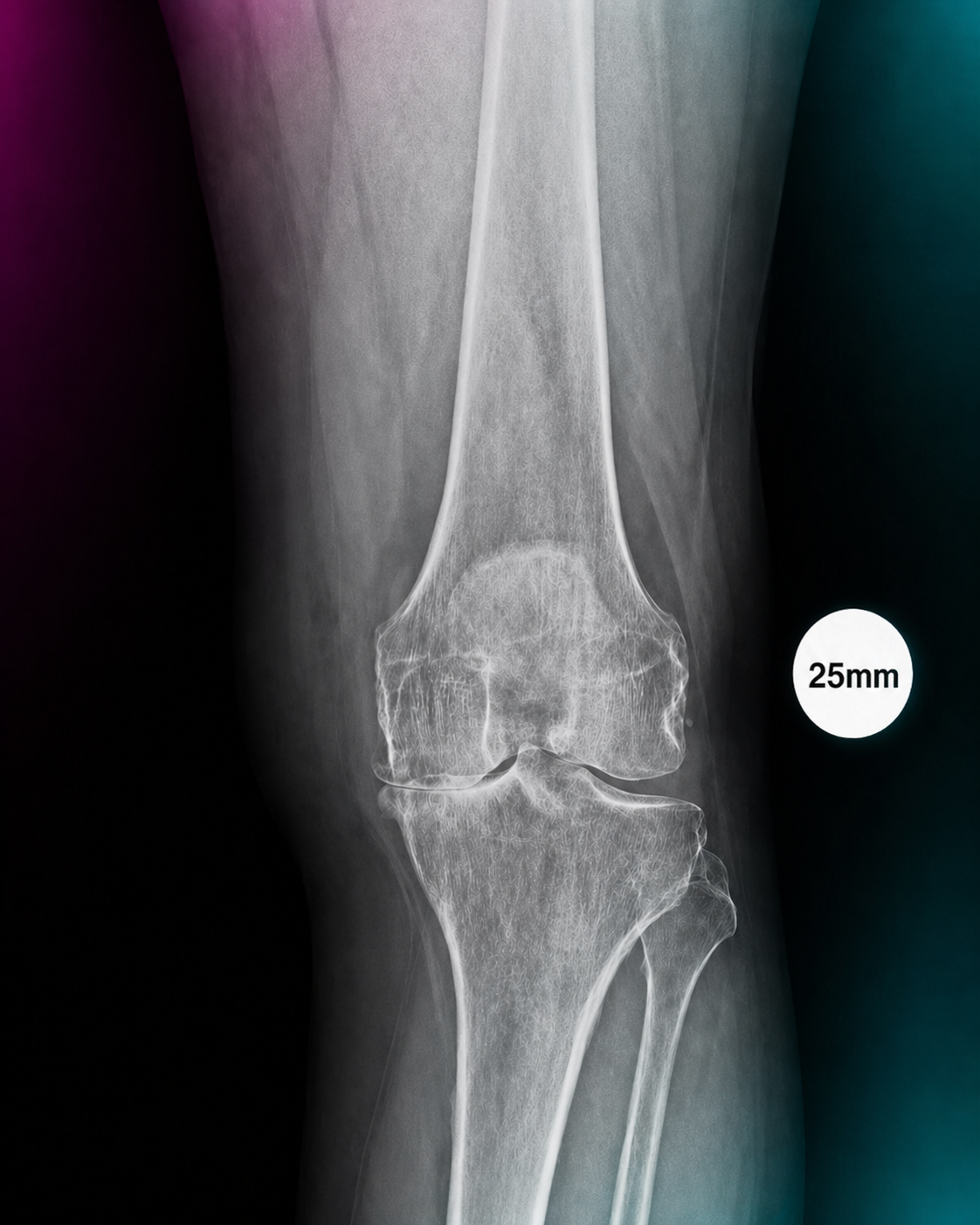
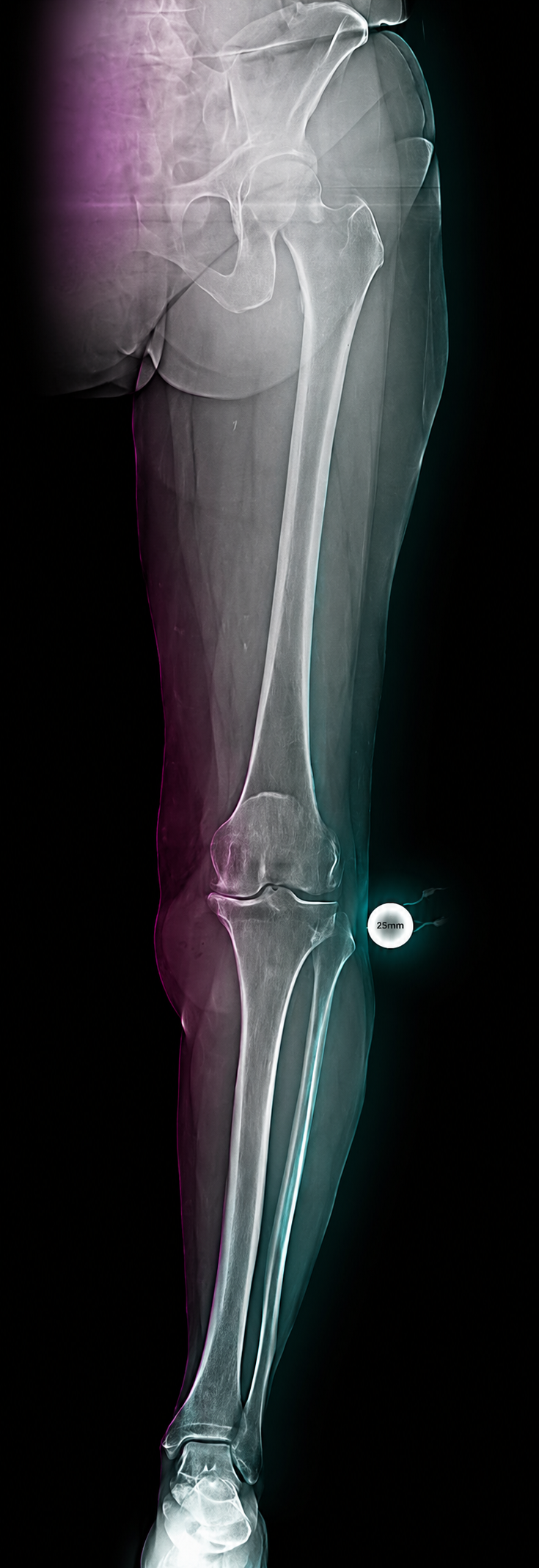
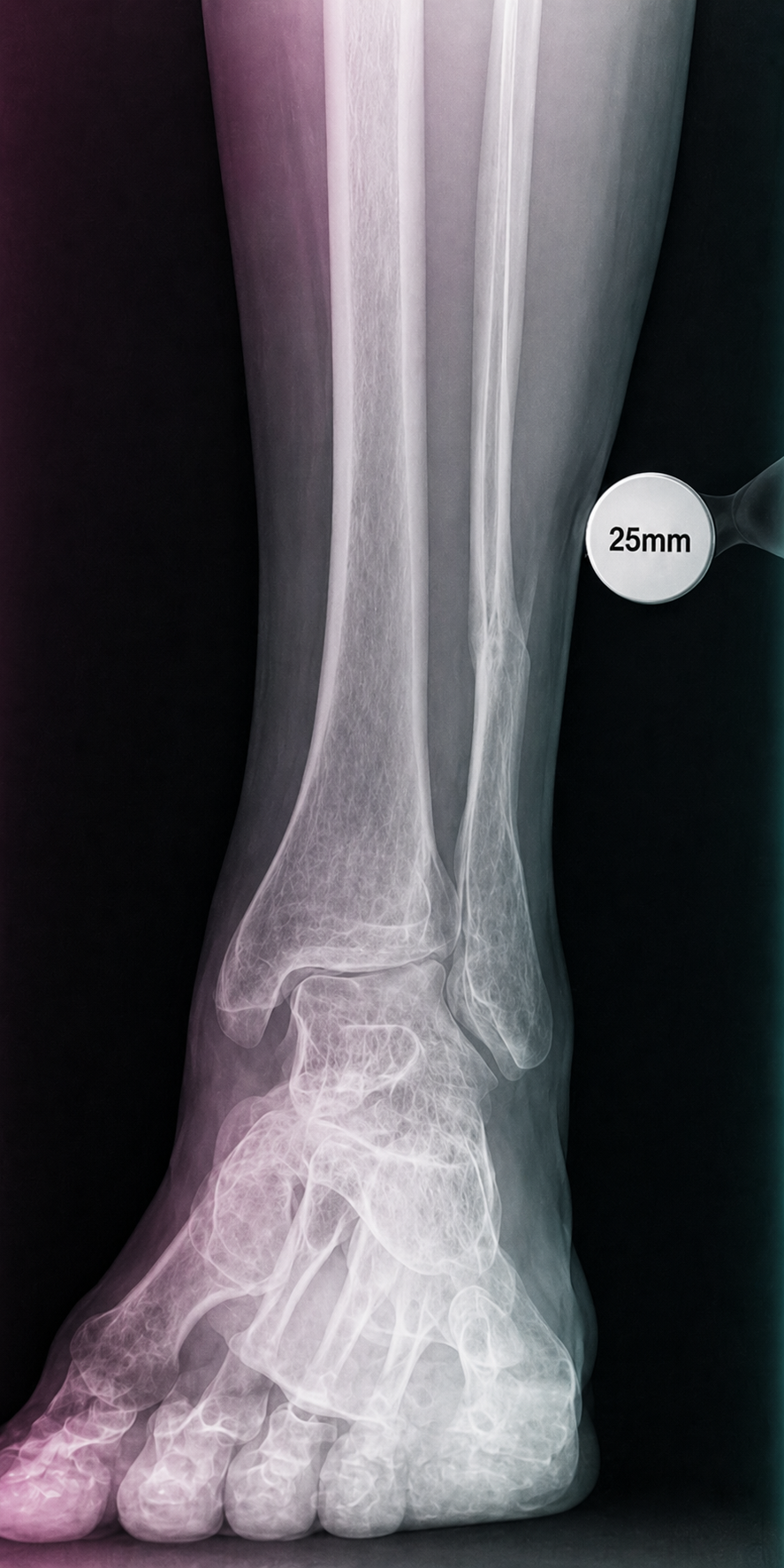
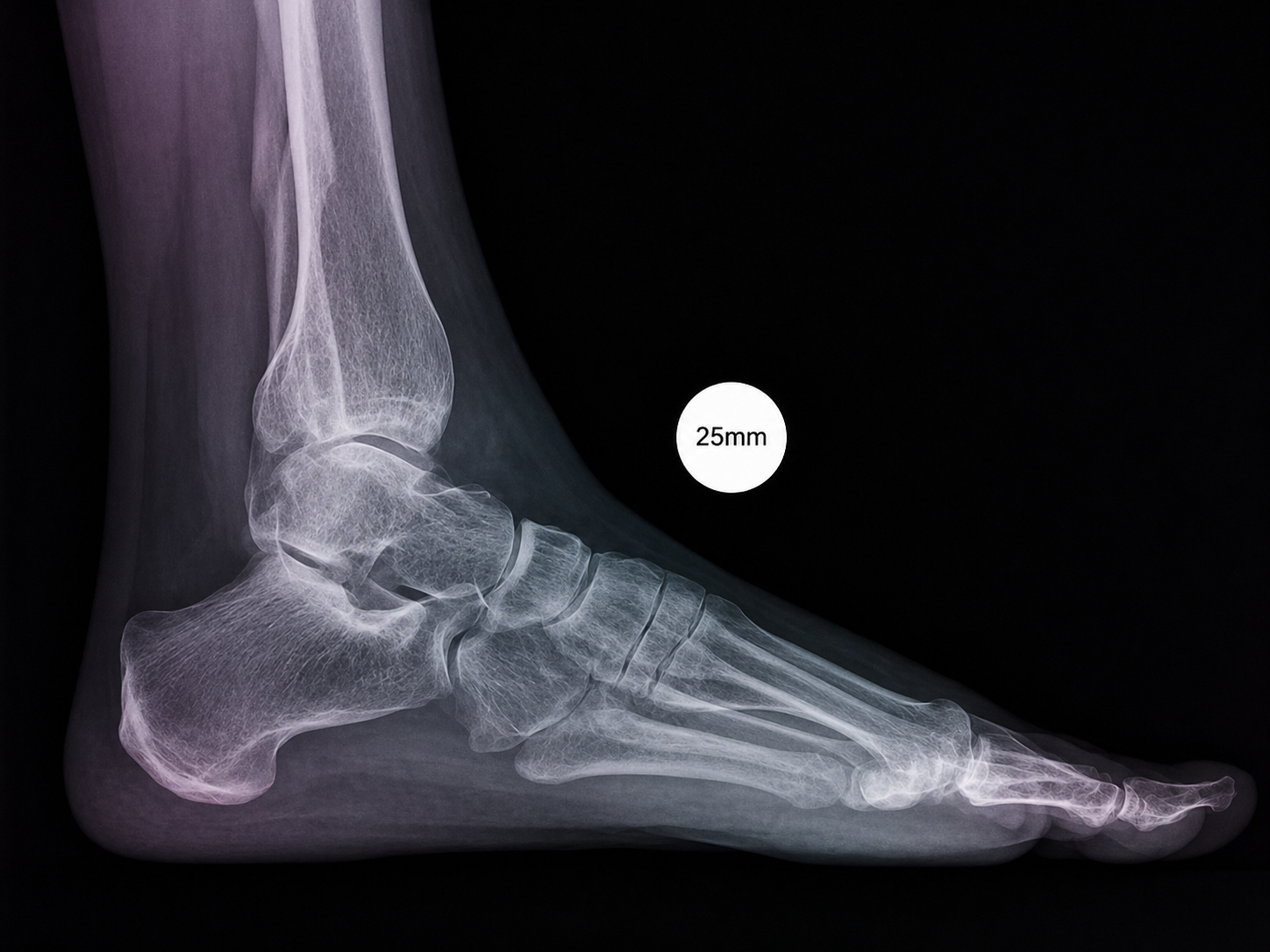
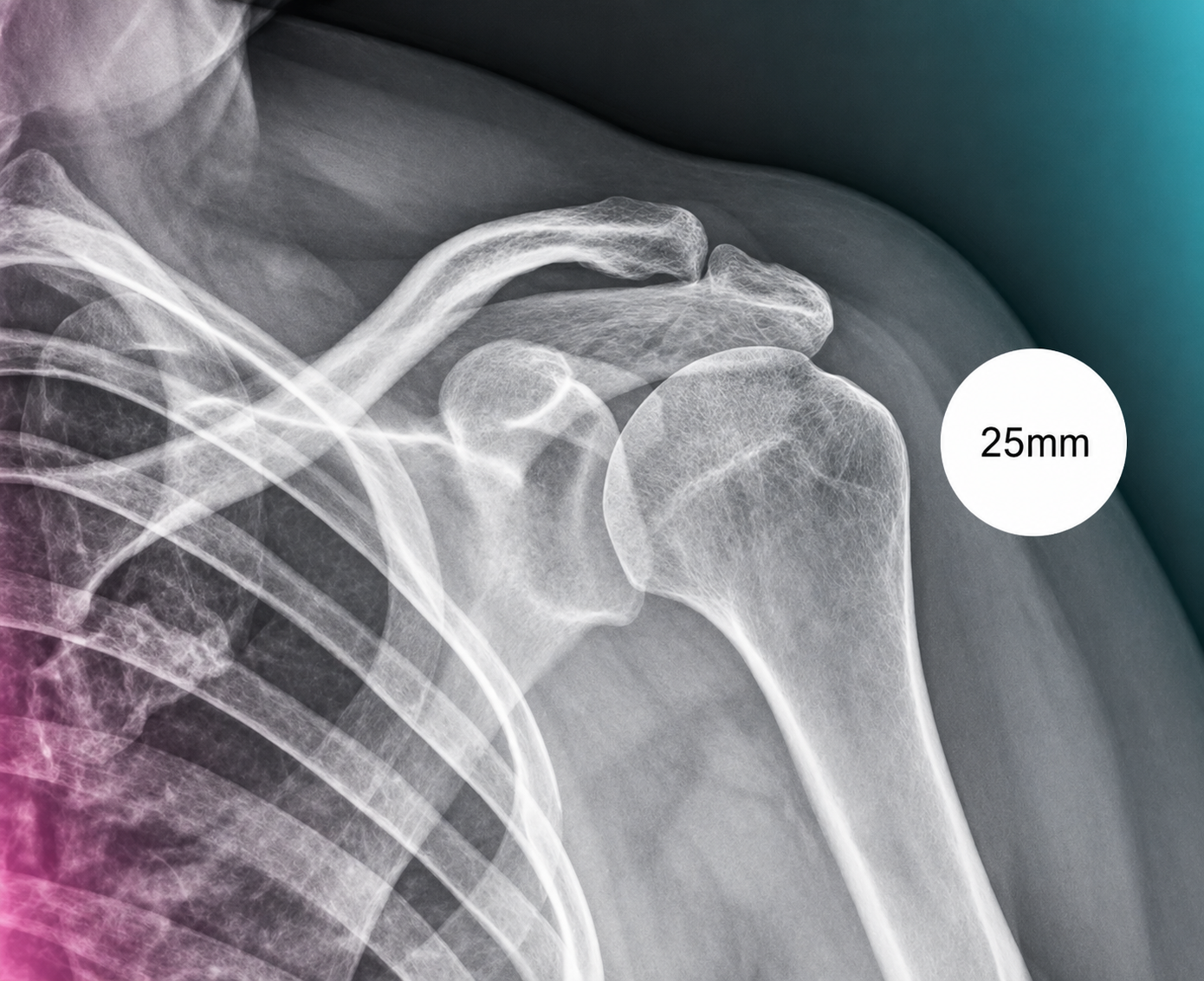
A compact guide for radiology teams on correct calibration sphere placement in orthopedic X-ray imaging. The marker must be positioned in the anatomical plane of the target joint so that digital scaling, measurements and preoperative templating remain clinically reliable.